The TheraRadar Brief
Every drug has multiple stories. Most never get told.
Casgevy Doesn’t Fix the Sickle Cell Mutation
It goes around it. That’s why it works.
Get the next TheraRadar Brief in your inbox
Drug development, biology, and market dynamics — free, every week.
Sickle cell disease is a single-letter typo in DNA. CRISPR can now edit DNA with precision. You'd think the fix is obvious.
It's not.
The typo
Sickle cell disease was identified as a molecular disease by Linus Pauling in 1949. Vernon Ingram pinpointed the exact defect in 1956 - one amino acid wrong in the HBB gene (glutamic acid → valine at position 6). It causes hemoglobin to polymerize into rigid fibers, deforming red blood cells into sickle shapes. Possibly one of the most understood genetic diseases in history.
CRISPR-Cas9 can now cut DNA at a precise location. The obvious approach: go to position 6 of HBB and correct the valine back to glutamic acid.
Casgevy (exagamglogene autotemcel) - developed by Vertex Pharmaceuticals and CRISPR Therapeutics, and approved by the FDA in December 2023 as the first CRISPR-based therapy ever, for patients aged 12 and older with sickle cell disease (SCD) - doesn't do this. It cuts a completely different gene. (A second indication, transfusion-dependent beta-thalassemia, was approved in January 2024.)
The workaround
Every human produces fetal hemoglobin (HbF) in the womb. After birth, a gene called BCL11A switches it off and adult hemoglobin (HbA) takes over. In sickle cell patients, the adult hemoglobin is broken - but the fetal hemoglobin was fine.
Doctors had known since the 1940s that some sickle cell patients had milder disease - the ones who naturally produced more fetal hemoglobin. But nobody knew what controlled the switch. You couldn't reactivate HbF if you didn't know what turned it off.
Stuart Orkin's lab at Harvard (2008) found the answer: BCL11A is the master switch. It's a transcription factor - a protein that binds to DNA and controls whether other genes are on or off. After birth, BCL11A silences the fetal hemoglobin gene cluster. Remove BCL11A, fetal hemoglobin comes back.
But there's a problem. BCL11A isn't only used in red blood cells. It's also critical for B-cell development in the immune system. Knock out BCL11A entirely and you fix the blood disease but cripple the immune system.
Bauer et al. (2013), working in Orkin's lab, solved this. BCL11A has different regulatory switches in different tissues. Bauer found an erythroid-specific enhancer - a stretch of DNA that only activates BCL11A in red blood cell precursors. Cut this enhancer, and BCL11A stops being produced in red blood cells (so fetal hemoglobin comes back) but still works normally in immune cells (because those use a different enhancer). Same gene, different control switch depending on cell type.
Casgevy uses CRISPR to cut this enhancer. BCL11A stops suppressing fetal hemoglobin in red blood cell precursors. Fetal hemoglobin comes back. It compensates for the broken adult hemoglobin.
They didn't fix the typo. They turned on the backup.
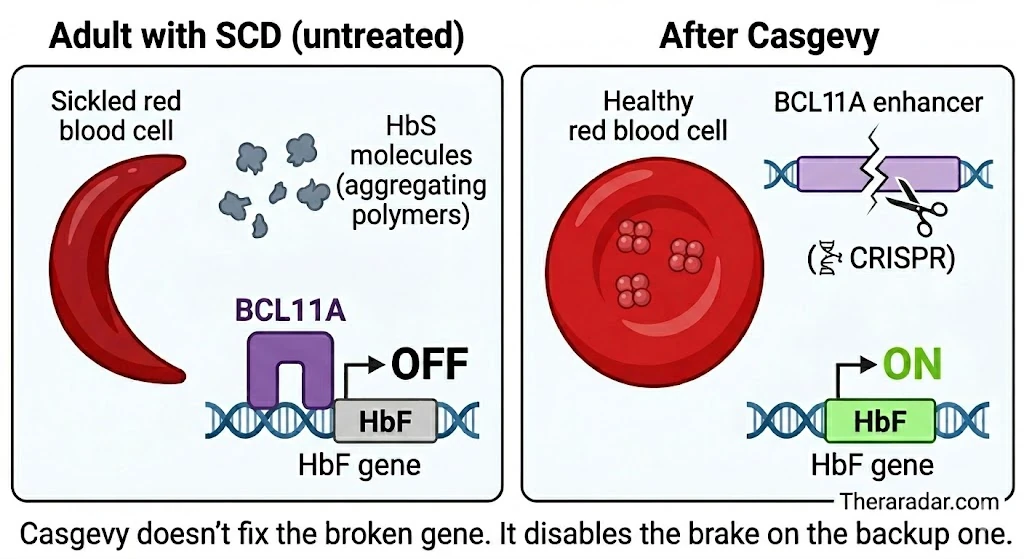
Theraradar. Casgevy doesn't fix the broken gene. It disables the brake on the backup one.
What's in the diagram
HbS (sickle hemoglobin) - the broken adult hemoglobin produced in SCD. Polymerizes into rigid fibers that deform red blood cells.
HbF (fetal hemoglobin) - the backup hemoglobin everyone produces before birth. Works fine; doesn't sickle. Its gene is silenced after birth.
BCL11A - a transcription factor. After birth it binds near the HbF gene cluster and shuts it off - the "brake" on the backup.
BCL11A enhancer - a stretch of DNA that tells the cell when and where to produce BCL11A. The erythroid-specific enhancer is the one active in red blood cell precursors.
CRISPR - cuts only the erythroid enhancer. BCL11A stops being made in red blood cells, so HbF reactivates. Immune cells use a different enhancer and are unaffected.
Why not fix it directly?
Correcting a point mutation with CRISPR requires a process called homology-directed repair (HDR). In hematopoietic stem cells, HDR efficiency has historically been 10-20% in the best cases - and even when editing works in the lab, HDR-edited cells engraft poorly after transplant. That's not enough to build a therapy on.
Casgevy uses the other repair pathway - non-homologous end joining (NHEJ) - which just needs a clean cut, no template. NHEJ efficiency in stem cells is 80-90%, and the edited cells engraft well. The choice between these two pathways is why Casgevy exists and a direct HBB correction doesn't - at least not yet.
From lab to license, in a decade
In 2012, Emmanuelle Charpentier and Jennifer Doudna published the Science paper showing CRISPR-Cas9 could be reprogrammed as a general-purpose genome-editing tool. They shared the 2020 Nobel Prize in Chemistry for it. Without this, none of what follows is possible.
In 2015, Vertex Pharmaceuticals partnered with CRISPR Therapeutics - the company Charpentier had co-founded two years earlier - on what would become CTX001. Vertex paid $105M up front plus up to $2.6B in milestones. The two companies brought different things: CRISPR Therapeutics contributed the editing science and the BCL11A-enhancer rationale; Vertex contributed the manufacturing scale, regulatory experience, and global commercial organization it had built over two decades of delivering the cystic fibrosis franchise (Kalydeco, Trikafta). By 2021 the economics had settled at Vertex 60% / CRISPR Therapeutics 40% of profits.
Most of the CRISPR world - Editas, Beam, Intellia - was chasing direct correction of disease genes. Vertex/CRISPR Therapeutics bet on the indirect path: cut the BCL11A enhancer, let fetal hemoglobin do the work. NHEJ worked in stem cells; HDR didn't. Bauer's enhancer gave them a clean, defined target. They got to FDA first. Lyfgenia - the direct-correction competitor approved the same day - carries a black-box warning for blood cancer.
The first patient was dosed in 2019. The New England Journal of Medicine published interim data in 2020. Breakthrough, RMAT, and Orphan designations followed. On December 8, 2023, the FDA approved Casgevy - the first CRISPR-based therapy for any disease. Eleven years from tool invention to an approved therapy; faster than most small molecules with a decade head start.
What the patient goes through
The science is elegant. The treatment is not. Casgevy requires extracting a patient's own stem cells, editing them in a lab, destroying the patient's existing bone marrow, and transplanting the edited cells back. It's a one-time treatment - but it takes roughly six months and the conditioning step is brutal.
- 1 Stem cell mobilization and collection (multiple sessions)
- 2 Cells shipped to manufacturing facility
- 3 CRISPR editing via electroporation (no viral vector)
- 4 Quality testing of edited cells
- 5 Myeloablative conditioning - patient's bone marrow wiped with busulfan chemotherapy (weeks in hospital, fertility risk, infection risk)
- 6 Edited cells infused back
- 7 Engraftment monitoring (4-6 weeks)
Total process: up to 9-12 months from first collection to recovery. The conditioning step - wiping the patient's existing bone marrow - is the hardest part.
The results
Sickle cell patients live with vaso-occlusive crises (VOCs) - episodes of extreme pain caused by sickled cells blocking blood vessels. Some patients experience them monthly.
A VOC is not a headache or a bad day. It is hours or days of deep bone pain - patients describe it as fractures from the inside - requiring emergency room visits, IV opioids, and hospital stays. Children with severe SCD miss weeks of school a year. Adults lose jobs. Some patients live through this cycle from childhood to death. The primary measure of whether Casgevy works is whether these crises stop.
| Measure | Result |
|---|---|
| SCD patients VOC-free | 100% (45/45) |
| Mean VOC-free duration | 35.3 months |
| Longest follow-up | 5.5+ years, still durable |
| Beta-thalassemia: transfusion independence | 98.2% (55/56), 6+ years follow-up |
Two approaches, same disease, same day
Casgevy wasn't the only gene therapy approved for sickle cell that day. On the same date - December 8, 2023 - the FDA also approved Lyfgenia (lovotibeglogene autotemcel) from bluebird bio.
Lyfgenia takes the direct approach. Instead of reactivating fetal hemoglobin, it uses a lentiviral vector to insert a modified hemoglobin gene - called βA-T87Q-globin - into the patient's stem cells. The resulting protein, HbAT87Q, differs from normal adult hemoglobin by a single amino acid out of 146 - a threonine-to-glutamine substitution at position 87, designed to physically block sickle hemoglobin from polymerizing into the rigid fibers that deform red blood cells.
Two companies, two technologies, two bets on how to solve the same disease.
Want the next brief? Subscribe — free, every week.
| Casgevy | Lyfgenia | |
|---|---|---|
| Approach | CRISPR gene editing (cuts BCL11A) | Lentivirus gene addition (adds working HBB copy) |
| What it does | Reactivates fetal hemoglobin | Produces modified adult hemoglobin (HbAT87Q) |
| VOC-free rate | 100% (45/45)* | 87.5% (28/32) |
| Price | $2.2M | $3.1M |
| Cancer risk | None observed | Black box warning - blood cancer cases |
| Delivery | Electroporation (no virus) | Lentivirus (integrates into genome) |
| FDA approval | December 8, 2023 | December 8, 2023 |
| Company | Vertex / CRISPR Therapeutics | bluebird bio |
*Casgevy VOC-free rate updated to latest data (ASH 2025, 45 patients). Lyfgenia data from original HGB-206 trial (32 patients). Different trial sizes and follow-up periods.
Both were approved the same day. Lyfgenia took the direct approach - adding a functional copy of the hemoglobin gene via lentivirus. It carries a black box warning for blood cancer risk because lentiviral vectors integrate at unpredictable locations in the genome - biased toward active genes - and can activate oncogenes. Casgevy cuts at a defined location and doesn't integrate anything, which is why its safety profile looks different. The direct approach is conceptually simpler. The indirect one is proving safer.
Access
- Only ~75 authorized treatment centers globally as of mid-2025
- ~115 patients have completed cell collection; only 29 have received infusions
- Vertex negotiated an outcomes-based payment deal with CMS - the first federal Medicaid program of its kind for gene therapy
- Expansion to children 5-11: regulatory submissions planned H1 2026
Possibly one of the most understood genetic diseases in history. A technology that can precisely edit any gene. And the therapy that works best goes around the broken gene entirely - reactivating a system that evolution built and then shut off. Sometimes the most elegant solution is the indirect one.
Go deeper with Pro
Pro gives you the data — patent cliffs, trial analytics, competitive landscapes, revenue tracking. Briefs tell the story with the data. Launch pricing: $99/month.
See Pro plansGet the next Brief in your inbox — free
Every drug has multiple stories. Most never get told. One brief every week. No spam.
Archive at /briefs/. Unsubscribe anytime.
Sources
- Pauling's 1949 paper: Pauling, Itano, Singer, Wells - "Sickle Cell Anemia, a Molecular Disease," Science (1949)
- CRISPR-Cas9 as a genome-editing tool: Jinek, Charpentier, Doudna et al., Science (2012)
- Nobel Prize in Chemistry 2020: Charpentier & Doudna - method for genome editing
- Vertex / CRISPR Therapeutics partnership: Vertex press release (October 2015)
- CTX001 NEJM interim data (2020): Frangoul et al., N Engl J Med (2021)
- Orkin lab BCL11A discovery: Sankaran et al., Science (2008)
- Bauer lab enhancer mapping: Bauer et al., Science (2013)
- FDA approval: FDA press release - first gene therapies for SCD
- PMC review: Casgevy approval review
- Mechanism of action: Casgevy HCP - mechanism of action
- Clinical trial results: Casgevy.com - SCD study information
- Longer-term data: Vertex EHA 2025 data presentation
- Dual breakthrough: PMC - Casgevy and Lyfgenia
- ACMG bulletin: ACMG therapeutics bulletin
- Business update: CRISPR Therapeutics Q2 2025 update
Spot an error? Reach out at hello@theraradar.com.