The TheraRadar Brief
Every drug has multiple stories. Most never get told.
KRAS: 40 Years Undruggable, Then Drugged. Then What?
It took 40 years to drug KRAS. The real competition started the day it worked.
Get the next TheraRadar Brief in your inbox
Drug development, biology, and market dynamics — free, every week.
KRAS is mutated in roughly 30% of all human cancers. It is the most common oncogene.
For 40 years, no one could drug it. Not for lack of trying - nearly every major pharmaceutical company attempted and failed. KRAS became the textbook example of an undruggable target.
Then, in 2013, a chemist found a hidden pocket that nobody knew existed.
The target
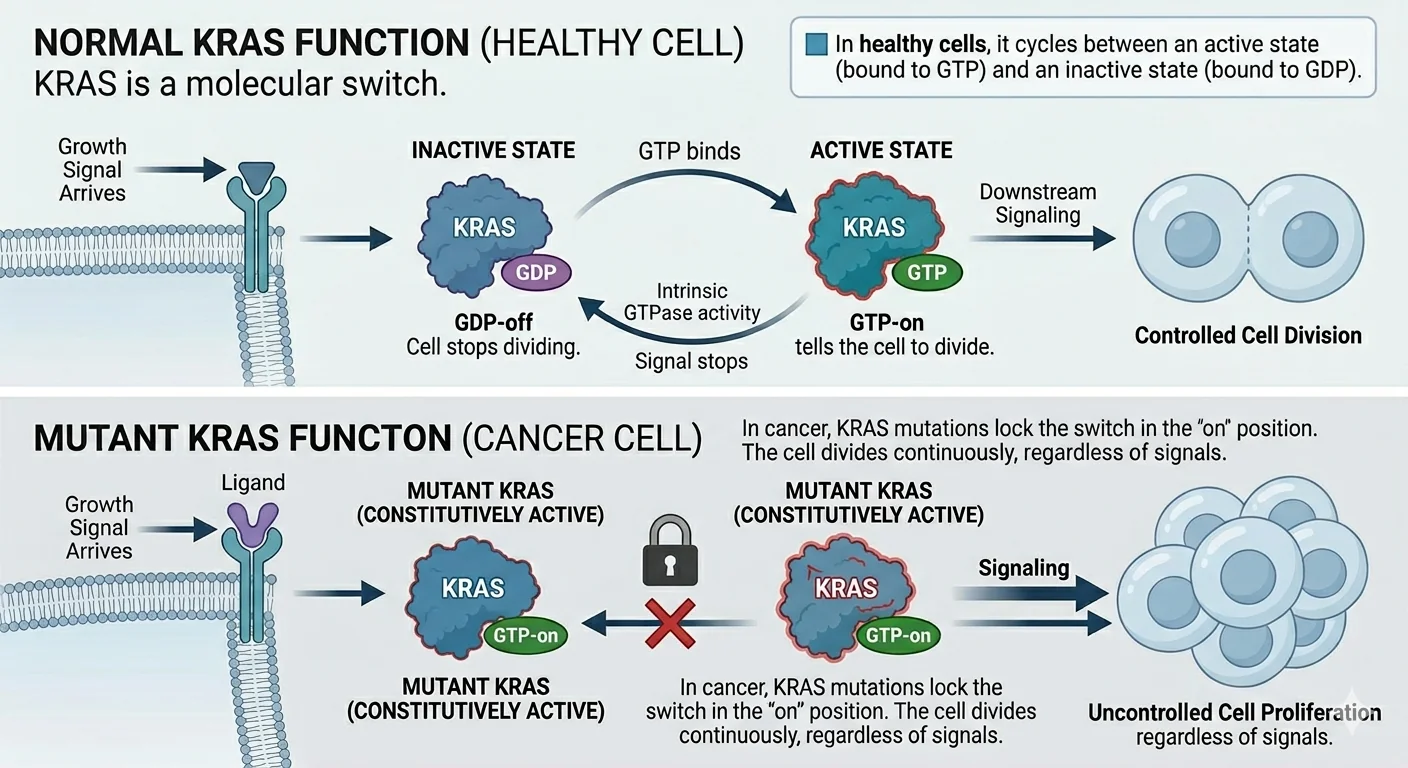
KRAS is a molecular switch. In healthy cells, it cycles between an active state (bound to GTP) and an inactive state (bound to GDP). When a growth signal arrives, KRAS flips to GTP-on and tells the cell to divide. When the signal stops, KRAS flips back to GDP-off and the cell stops dividing.
In cancer, KRAS mutations lock the switch in the "on" position. The cell divides continuously, regardless of signals. The most common of these mutations - G12C, G12D, G12V - change a single amino acid at position 12, jamming the switch.
KRAS G12C is found in roughly 13% of non-small cell lung cancers, 3-5% of colorectal cancers, and 1-2% of pancreatic cancers. These are not rare cancers. Across all tumor types, KRAS mutations appear in roughly one in every five to six cancer patients.
Why it was undruggable
Most small-molecule drugs work by fitting into a pocket on the target protein - like a key in a lock. KRAS has no obvious pocket. Its surface is smooth and featureless. The protein is small (21 kDa), tightly folded, and binds its natural substrate (GTP) with picomolar affinity - meaning any drug would need to compete with a molecule the protein holds a trillion times tighter than most drug-target interactions.
For decades, researchers tried to block KRAS from the outside, target proteins downstream of KRAS, or prevent KRAS from reaching the cell membrane. None of these strategies produced an approved drug. The National Cancer Institute launched a dedicated RAS Initiative in 2013, reflecting both the importance of the target and the frustration of the field.
How a UCSF chemist cracked the pocket
In 2013, Kevan Shokat's lab at UCSF published a paper in Nature that changed the field. They discovered something no one had seen in three decades of studying KRAS: a pocket.
The pocket - called the switch II pocket - does not exist in normal KRAS. It only forms in the G12C mutant, and only when the protein is in its inactive (GDP-bound) state. The G12C mutation replaces glycine with cysteine at position 12. Cysteine has a sulfur atom - a reactive handle that a drug can grab onto permanently through covalent binding.
Shokat's group designed compounds that slip into this pocket and form an irreversible bond with the mutant cysteine. Once bound, the drug locks KRAS in its inactive state. The switch cannot flip back on. The cancer signal stops.
The elegance of this approach is its selectivity. Normal KRAS (with glycine at position 12) does not have the cysteine, so the drug cannot bind to it. The drug hits only the mutant protein in tumor cells and leaves the normal protein in healthy cells untouched.
RAS oncogenes identified in human cancers
First link between RAS mutations and human tumors
30 years of failed attempts
No binding pocket. No approved drug. "Undruggable" label sticks.
Shokat co-founds Araxes Pharma / Wellspring Biosciences
UCSF chemist Kevan Shokat starts a company to develop his own discovery. Partners with Janssen (J&J) in an exclusive deal.
Shokat lab publishes the Switch II pocket (Compound 12)
A hidden allosteric pocket that only opens in the G12C mutant. The paper launches a global race.
Three independent programs race on the same pocket
Wellspring/J&J: Compound 12 → ARS-853 → ARS-1620 (first in vivo activity). Amgen: develops AMG-510 independently. Mirati: develops MRTX849 independently.
Amgen's AMG-510 enters Phase I first (July 2018)
Amgen beats the discoverer's own company to the clinic.
ASCO 2019: first patient responses - standing ovation
AMG-510 shows tumor shrinkage in NSCLC patients. Mirati's MRTX849 enters Phase I. Wellspring/J&J's ARS-3248 also enters clinic.
J&J drops ARS-3248 in Phase I - muscle toxicity, only 10 patients
Severe muscle damage (elevated CPK) at effective doses. Tolerable doses too low to work. Never reached dose expansion. The discoverer's own compound didn't make it - while Amgen and Mirati, using the same pocket he found, advanced.
Lumakras (sotorasib) - FDA accelerated approval
Amgen wins the race. First drug ever approved to directly target KRAS.
Krazati (adagrasib) - FDA accelerated approval
Mirati comes second. BMS later acquires Mirati for $5.8 billion.
FDA ODAC votes 10-2 against Lumakras full approval
CodeBreaK 200: PFS met, but OS missed. Study integrity concerns. Lumakras stays on accelerated approval.
Next generation: beyond G12C
Divarasib (Roche): 13.8mo PFS, Phase III. Zoldonrasib (Revolution Medicines): G12D, 61% ORR, FDA BTD. Daraxonrasib (Revolution Medicines): Phase 3 RASolute 302 in 2L metastatic PDAC reports 13.2 vs 6.7mo OS (HR 0.40, April 2026). Pan-KRAS degraders entering trials.
TheraRadar.com
Same pocket, different chemistry, different fates
All three compounds share the same basic architecture: an acrylamide warhead (the covalent "lock") on a pyrimidine-piperazine scaffold from Shokat's ARS-1620. The differences are in the molecular details.
| Sotorasib (Amgen) | Adagrasib (Mirati/BMS) | ARS-3248 (Shokat/J&J) | |
|---|---|---|---|
| Binding strategy | Weak reversible + strong covalent lock | Strong reversible grip + weaker covalent | Inherited from ARS-1620 lineage |
| Half-life | ~5 hours | ~23 hours | Never established |
| H95 dependence | Low - works across RAS isoforms | High - KRAS-specific | Unknown |
| Key toxicity | Liver enzyme elevation | GI symptoms, fatigue | Skeletal muscle damage |
| Outcome | FDA approved (2021) | FDA approved (2022) | Dropped in Phase I (10 pts) |
The lesson: discovering the target does not guarantee the best drug. Amgen and Mirati read the same 2013 paper, targeted the same pocket with the same warhead chemistry, but designed their own scaffolds - and avoided the toxicity that killed the discoverer's compound.
Because the two surviving drugs bind the pocket differently, they have complementary resistance profiles. Mutations at H95 that resist adagrasib have no effect on sotorasib. Conversely, G13D and A59S mutations that resist sotorasib remain sensitive to adagrasib. Two drugs that look similar on paper may turn out to be sequential treatment options.
Lumakras
sotorasib
| Company | Amgen |
| FDA approval | May 2021 |
| Trial | CodeBreaK 100 |
| Response rate | 37% |
| Median PFS | 5.6 months |
| Half-life | ~5 hours |
| CNS penetration | Limited |
| FY revenue | ~$300M/year |
Accelerated approval. Full approval rejected by ODAC (Oct 2023). New confirmatory study required by Feb 2028.
Krazati
adagrasib
| Company | BMS (acq. Mirati, $5.8B) |
| FDA approval | Dec 2022 |
| Trial | KRYSTAL-1 |
| Response rate | 43% |
| Median PFS | 5.5 months |
| Half-life | ~23 hours |
| CNS penetration | Yes - intracranial responses |
| FY-2025 revenue | $205M |
Critical for ~30% of NSCLC patients whose cancer spreads to the brain. Sotorasib cannot reach.
Both outperform standard chemotherapy in second-line NSCLC (5-6 months PFS vs 3.8-4.5 for docetaxel). For patients who respond - 37-43% in trials - the benefit can last 10-12 months, far longer than the median suggests. But resistance remains the central challenge: tumors adapt through secondary KRAS mutations, bypass pathway activation, or histological transformation. These are first-generation drugs for a target the field spent decades unable to touch at all.
Want the next brief? Subscribe — free, every week.
The commercial reality
The science delivered two approved drugs. The commercial reality proved more complicated.
Revenue from Amgen SEC filings via TheraRadar.
TheraRadar.com
Lumakras generates roughly $300 million a year. For context, Keytruda - the PD-1 inhibitor that Lumakras patients typically receive before or alongside - generated $29.5B in 2024. Lumakras is roughly 1% of Keytruda's revenue, treating a subset of the same patient population.
Several factors explain the gap between scientific achievement and commercial performance:
- Small addressable population. KRAS G12C appears in ~13% of NSCLC patients. Of those, most receive Lumakras only after progressing on prior therapy. The eligible population at any given time is limited.
- The confirmatory trial stumbled. CodeBreaK 200 compared sotorasib to docetaxel in second-line NSCLC. It met its primary endpoint (progression-free survival), but showed no improvement in overall survival. An FDA advisory committee voted 10-2 in October 2023 that the PFS results could not be reliably interpreted, citing potential bias from differential dropout rates. The FDA issued a Complete Response Letter, rejecting full approval. Lumakras remains on accelerated approval, with a new confirmatory study required by February 2028.
- Competition from checkpoint inhibitors. Keytruda-based combinations dominate first-line NSCLC treatment. By the time patients progress to second-line where Lumakras is used, many have limited options and limited time - narrowing the commercial window.
Why the science still matters
The commercial disappointment of first-generation KRAS G12C inhibitors does not diminish what they proved: KRAS is druggable. The pocket exists. The covalent chemistry works. The selectivity is real. What did not work was the clinical context - second-line monotherapy in a market dominated by immunotherapy combinations.
Who benefits most: the biomarker picture
Biomarker data is revealing which patients gain the most from KRAS G12C inhibitors - and which don't. Patients with STK11 co-mutations - who respond poorly to immunotherapy - show response rates as high as 64% on KRAS G12C inhibitors (KRYSTAL-1 subgroup analysis). These are exactly the patients with the fewest other options. Conversely, KEAP1 co-mutations predict poor response (14-29%), emerging as the key negative biomarker (Journal of Translational Medicine, 2025).
The median duration of response for those who do respond is 10-12 months - far longer than the 5-6 month median PFS suggests, because the median is dragged down by non-responders.
Next-gen G12C: divarasib (Roche)
Divarasib (Roche/Genentech) is a next-generation G12C inhibitor with 5-20x higher potency than sotorasib. In a Phase I study of 60+ NSCLC patients, it showed a 56% response rate and 13.8 months median PFS - nearly triple the first-generation numbers. Its Phase III trial (KRASCENDO-1), a head-to-head comparison against sotorasib and adagrasib, reads out in 2026.
Beyond G12C: zoldonrasib and daraxonrasib (Revolution Medicines)
Revolution Medicines is leading on the mutations that first-generation drugs cannot touch. Zoldonrasib (RMC-9805) targets KRAS G12D - the mutation most common in pancreatic cancer, which has zero approved targeted therapies. It received FDA Breakthrough Therapy Designation in January 2026 after showing a 61% response rate in KRAS G12D-mutated NSCLC. Breakthrough Therapy Designation means the FDA saw data compelling enough to accelerate review; roughly 60-70% of drugs that receive it eventually get approved, compared to ~10-15% of all drugs entering trials.
Daraxonrasib (RMC-6236) is a multi-selective RAS inhibitor designed to work across multiple KRAS mutations - potentially addressing the full 30% of cancers with RAS alterations rather than the ~2% with G12C. In April 2026, the Phase 3 RASolute 302 trial in previously treated metastatic pancreatic cancer reported a median overall survival of 13.2 months versus 6.7 months on investigator's-choice chemotherapy (HR 0.40, p<0.0001) - roughly a doubling of survival in a disease where every prior targeted therapy has failed, and across a population that included RAS G12D, G12V, G12R, and RAS wild-type tumors.
Kevan Shokat - the UCSF chemist whose 2013 paper opened the field - is an academic co-founder of Revolution Medicines and a member of its scientific advisory board. After ARS-3248 failed at his first venture (Araxes/Wellspring), his second company is now leading the next generation.
After note (May 2026): The Phase 1/2 results that justified the Phase 3 design were published in the New England Journal of Medicine, and on May 1, 2026 the FDA issued a "safe to proceed" letter authorizing an expanded access protocol for previously treated metastatic PDAC - signed just two days after the request was received.
Pan-KRAS degraders: destroy the protein entirely
A third approach is emerging: pan-KRAS degraders that destroy the KRAS protein rather than just blocking it. Multiple programs are entering clinical trials, aiming to work regardless of which KRAS mutation is driving the tumor. The shift from one mutation, one drug, one setting to broad RAS inhibition across cancer types is the real story now.
The bottom line
Forty years of failure. One hidden pocket. Two approved drugs - and a pipeline that suggests they were just the beginning. Lumakras stalled commercially, but Krazati's brain penetration advantage, BMS's $5.8 billion bet, Roche's next-gen data tripling PFS, Revolution Medicines' breakthrough into G12D, and daraxonrasib doubling overall survival in second-line pancreatic cancer all signal that the market hasn't given up on KRAS. The target is cracked open. The question is whether next-generation drugs can turn a proven mechanism into a blockbuster.
Go deeper with Pro
Pro gives you the data — patent cliffs, trial analytics, competitive landscapes, revenue tracking. Briefs tell the story with the data. Launch pricing: $99/month.
See Pro plansGet the next Brief in your inbox — free
Every drug has multiple stories. Most never get told. One brief every week. No spam.
Archive at /briefs/. Unsubscribe anytime.
Sources
- Switch II pocket discovery: Ostrem et al., Nature (2013)
- Lumakras approval: FDA accelerated approval (May 2021)
- CodeBreaK 200 / ODAC: FDA ODAC vote (Oct 2023)
- Zoldonrasib BTD: Revolution Medicines press release (Jan 2026)
- KRAS mutation prevalence: Arbour et al., JCO Precision Oncology (2022)
- Revenue data: Amgen and BMS SEC filings via TheraRadar
- STK11 co-mutation response (64% ORR): KRYSTAL-1 STK11 subgroup, Targeted Oncology
- KEAP1 as negative biomarker: Journal of Translational Medicine (2025)
- Divarasib Phase I (56% ORR, 13.1mo PFS): Li et al., NEJM (2023)
- Sotorasib vs adagrasib binding specificity: ACS Chemical Biology (2024)
- ARS-3248 Phase I (muscle toxicity): The Oncologist (2022)
- KRAS G12C inhibitor clinical history: J Exp Clin Cancer Res (2022)
- Pan-KRAS degraders: Science (2024)
Spot an error? Reach out at hello@theraradar.com.